clinical emergency medicine, critical medical anthropology
Author: Jason Wilson, MD, PhD, CPE, FACEP
Jason Wilson, MD, PhD, CPE, FACEP is an emergency physician, academic healthcare leader and medical anthropologist with an interest in developing patient-centered pathways that are medically efficacious but also consider the role of structural and cultural forces in determining health inequities and disparities.
TAMPA, Fla. — Tampa General Hospital and USF Health are part of a nationwide study that is looking at older medications to treat COVID-19.
“So ACTIV-6 is for those re-purposed drugs that have at least enough evidence behind them that says there might be a signal here that can help somebody, but more importantly, everything that has been done with them so far, there’s really not a signal for harm. And so to make it into the ACTIV-6 group of drugs that might be used, re-purposed, you have to at least meet that level of safety and possible efficacy against NIH study. So that means the bar is very high. The bar is very high for making sure we’re doing the study,” explained Dr. Jason Wilson.
The study will look at drugs (ivermectin, fluticasone furoate, and fluvoxamine) to see their impact on the omicron variant of COVID-19. The drugs will be taken in an outpatient setting, which means you won’t have to leave your house. Right now, there are no FDA-approved drugs to treat mild to moderate symptoms of COVID-19, which this study hopes to look at.
“We’re looking just like with vaccines, to see if we can keep people out of the hospital, or keep people from dying from COVID. And that’s really about the ACTIV-6 studies looking at prevention of hospitalizations by using repurposed drugs,” explains Dr. Wilson
Here are the qualifications you have to meet once you test positive for COVID-19 to participate in the study:
At least 30 years old and not pregnant
Tested positive within 10 days
Have at least two symptoms for seven days or less
Fatigue, difficulty breathing, fever, cough, nausea, vomiting, diarrhea, body aches, chills, headache, sore throat, nasal symptoms, loss of taste or smell
Once you enter the study, drugs will be sent to your house the next day. You will take them for a few days and the medical team will follow up for a month at different intervals of time. The communication will be via phone calls/mail. The drugs are free and you will be compensated $100.
“So the way this trial is designed, is that we’re going to capture thousands of people throughout the country. And we’re going to do it fairly quickly because there’s so many different trial sites. And it’s important to note too, that with ACTIV-6 some sites came online earlier, and some are just ramping up, like us. So the ones who came on earlier had some good tests around the delta variant. And as we come along, we’re getting a good test on omicron. The data we’re going to get it’s going to be really powerful for looking at that. But with four arms, meaning placebo, fluvoxamine, ivermectin, fluticasone. We got to have a lot of people in there to get good samples. So we’re hoping to enroll well into the hundreds in this area, and in the 1000s, in the state of Florida,” explained Dr. Wilson.
Click here for more information on the ACTIV-6 study and to find out how to enroll.
The University of South Florida and Tampa General Hospital have joined onto a nationwide study to look at existing medications as possible treatments for COVID-19 infections.
According to the ACTIV-6 study’s website, the Duke Clinical Research Institute coordinating the study along with Vanderbilt University Medical Center.
To be eligible for the study, an individual must be at least 30 years old, have tested positive for COVID-19 within the past 10 days and have at least two symptoms, including fatigue, difficulty breathing, fever, couch, and nausea, among others.
ACTIV-6 is a nationwide double-blind study that is expected to eventually have nearly 15,000 participants. People can participate from any part of the United States via the study’s website or by calling 833-385-1880.
Medications currently being studies include fluvoxamine, a selective serotonin reuptake inhibitor; fluticasone, an inhaled steroid; and ivermectin, which is used to treat parasitic infections.
USF’s Dr. Jason Wilson said participants will not have to leave their homes to be a part of the study.
“If you decide to take part in our study, our team reaches out to you, we have a conversation and get you medicine delivered the next day to your house in the mail,” he said. “So, really all the encounters will happen by phone and by mail, and you’ll always have that research team available to answer your questions.”
The purpose of the ACTIV-6 research study is to test medications that are already approved for other diseases to see if they can help people with mild to moderate COVID-19 feel better faster and stay out of the hospital. ACTIV-6 is part of the Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) program.
Patients are able to self-enroll in ACTIV-6 at activ6study.org
Patients that enroll in ACTIV-6 can still receive other outpatient therapies including Mabs, remdesvir, Paxlovid, and MolnupiravirACTIV-6 includes arms for fluvoaxmine, fluticasone, ivermectin, placebo
adults, Covid+ last 10 days, do not have to come in, do not have to have been seen at TGH/USF
There is a .ACTIV6 smart phrase with text from an IRB approved recruitment flier under the Epic User Name Wilson, Jason [18448]. That can be included in the AVS for the patient and used forreference
Nirmatrelvir+Ritonavir [Paxlovid]
Paxlovid can be found in Epic but requires you to search the database. Below are some screenshots for locating Paxlovid.
You can add it to your favorites when you order the medicine the first time.
You should then be able to find it easier the next time
Paxlovid CrCl > 60 ml/min
Paxlovid CrCl 31-60 ml/min
You can select the pharmacy during the ePrescribe process by clicking on the current pharmacy name (this example has TGH Outpatient Pharmacy).
TGH Outpatient Pharmacy does not have Paxlovid.
Only retail pharmacies have been supplied medication.
Information about Nirmatrelvir+Ritonavir [Paxlovid]
nirmatrelvir is a protease inhibitor that inhibits mPRO and stops viral replication EPIC-HR Trial (n=2,246).
28 day hospitalization in Paxlovid arm 0.8% (n=8), 6.3% in placebo arm (n=66). Relative Risk Reduction = 88%, Absolute Risk Reduction = 5.5%, Number Needed to Treat to prevent 1 hospitalization on Paxlovid = 18
All cause 28 day mortality Paxlovid arm 0%, placebo arm 1.1% (n=12). RRR = 100%, ARR = 1.1%
Number needed to Treat to prevent 1 death on Paxlovid = 91
Non-pregnant, adult patients can potentially receive Fluvoxamine as part of ACTIV-6. However, if patient does not want to join research study or definitively wants/needs Fluvoxamine, this is reasonable given clinical data to prescribe.
Clinical trial dosing was 100mg PO BID X 10 days (this is moderately large dose and can be associated with nausea; consider giving ondansteron RX with Fluvoxamine RX
Possible drug interactions (from the prescribing information which can be found at this link) with BZD, clozapine, methadone, mexiltine, antipsychotics, ramelton, theophyline, warfarin, NOACs, carbamazepine, sumatriptan, TCAs, tacrine, tryptophan, diltiazem, propranolol, metoprolol
Sotrivimab and Remdesvir
There is limited effectiveness of Eli-Lilly and Regeneron monoclonal antibody infusions for Omicron based on lab based studies.
Sotrovimab does have effectiveness against Omicron but there is very limited availability of the medication and requires high risk/immunocompromised conditions to access.
remdesvir is also available as outpatient but also requires high risk features and 3 days of return encounters.
Sotrovimab and remdesvir can be given in the GEDI at TGH to very high risk patients.
Patients and community providers can complete the referral form themselves.
TGH emergency medicine providers/TGH providers can utilize the AMB REFERRAL TO COVID 19 FOLLOW UP.
Sotrovimab and remdesvir referrals to GEDI from TGH/USF System can be made using the AMB Referral to Covid-19 Follow UpPatients must be high risk for sotrovimab or remdesvir infusion.
Epic Smart Phrase For All Outpatient Treatments and Risk Score for Mabs/Infusions
Other Outpatient Covid Treatment Options(USF Medicine, NIH, Collected Guidelines)
Non-Pregnant Patients
Vitamin D 5,000 units daily
encourage hydration
recommend prone positioning at home every 1 hour every 4 hours
Pregnant Patients
Can still be offered Vitamin D
Can be offered inhaled budesonide
Should not be prescribed fluvoxamine, molnupiravir, or paxlovid and are not eligible for ACTIV-6
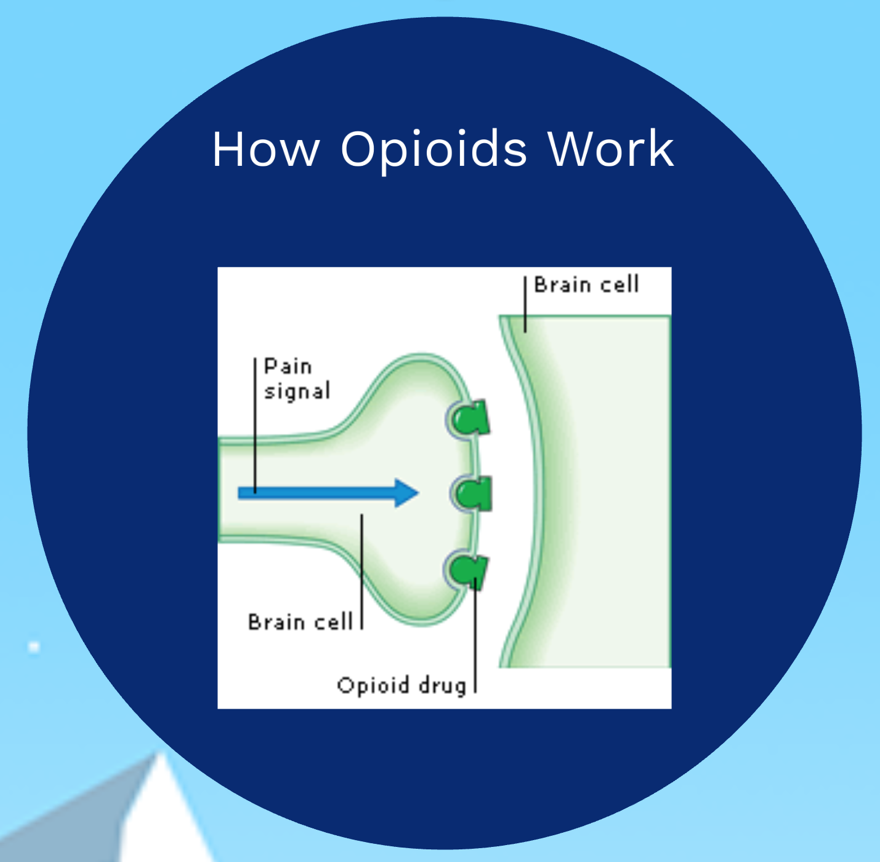
USF EM focuses on the assemblage of new care pathways through direct engagement and involvement of social scientists. We place social scientists (anthropologist) into the clinical space. This work has been best exemplified by our efforts to conduct non-targeted HIV and HCV screening and linkage to care, as well as the construction and implementation of an opioid use disorder bridge program utilizing buprenorphine, and the operation of a prehospital/out of hospital space syringe exchange program that moves us closer to a regional coordinated harm reduction system.
Our USF EM SEM team also have worked to vaccinate refugees, explore vaccine hesitancy in the ED, and investigate healthcare disparities and inequity in female health, including differential rates of endometrial cancer and potential opportunities for ED screening/intervention.
Jason Wilson, Roberta Baer and Seiichi Villalona are pleased to announce publication of our article in Academic Medicine which highlights the success we have had implementing a premed patient shadowing program that builds in a patient experience perspective into the preclinical years at the University of South Florida. The article is available for free at the Academic Medicine website.
Patient shadowing early in training allows a shift in the clinical gaze that pays off in the long game in the development of future physicians
Presented at the Society for Applied Anthropology
(TH-160) THURSDAY 5:30-7:20, April 6, 2018
CHAIR: WILSON, Jason (TGH, USF)
Opening Remarks
A gap exists between patient and provider expectations during healthcare encounters in the United States. Those gaps are especially prevalent in acute clinical settings such as the emergency department where physicians have a defined agenda to rule out life threatening disease within a small amount of time usually with a patient they do not know from previous visits. Sometimes the underlying reason for the ER visit is emergent and sometime it is not, sometimes the underlying reason is medical and sometimes it is not.
Arthur Klieinman framed the patient-physician gap over 30 years ago as a difference in explanatory models of disease and illness. Medical anthropologists have focused on the tension between biomedical and lay person models of health. However, the patient experience, as measured by healthcare surveys of satisfaction, has not improved significantly and may be even worse in a setting of overcrowded department, confusing healthcare insurance issues, and disjointed attempts at continuity.
Attempts to measure the existing gap between an ideal patient experience and the current state were formalized by Irwin Press in the 1980s with the now ubiquitous utilization of the Press-Ganey Survey. However, just because a phenomenon is measured does not mean that the problem is resolved.
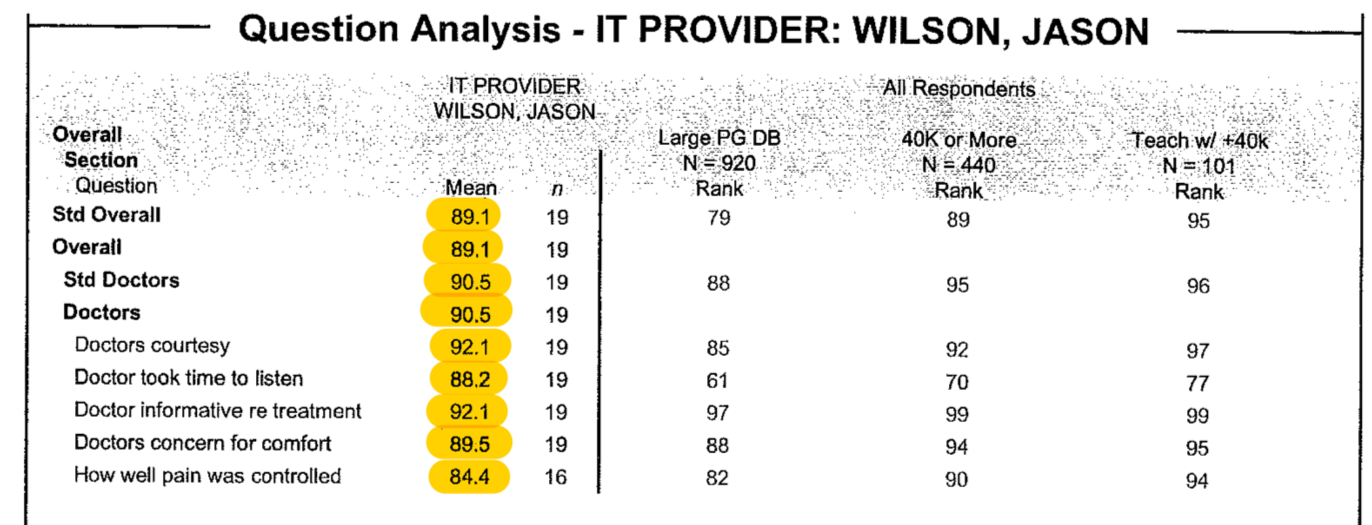
Hospitals spend millions to improve the patient experience, or at least to improve scores on patient satisfaction surveys. Those scores are now tied to reimbursement and the proportion of reimbursement related to those scores will only increase for providers and facilities moving forward.
What do hospitals get for all of this spending on patient satisfaction? Essentially everyone achieves mediocrity. The spread around the mean of these scores is incredibly tight. Moving from 83% to 85% might move you from the 50th percentile to the 90th percentile. The first large spend on patient experience by healthcare facilities is to ensure 50th percentile – drop below that and you risk a loss of federal reimbursement. The goal, however, is to ultimately move above average since that is where the rewards for higher patient satisfactions scores exist. Thus, hospitals spend incredible amounts of money to improve a few percentage points but, as the score gets higher the ability to increase the score by another percent also becomes exponentially more expensive.
Four years ago, a medical anthropologist and an emergency medicine physician decided to approach this issue together by repositioning the role of medical anthropology education in the premedical school curriculum as well as to position medical anthropologists as the obvious human resource for a healthcare organization patient experience department. As an ER doc who also went through the same training as our current students are just embarking upon, it was important to me to provide access to shadowing and research opportunities but with enhanced student engagement.
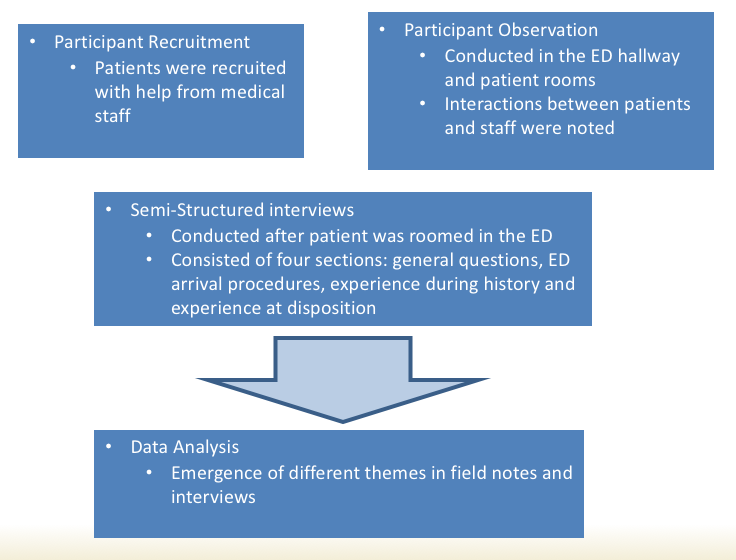
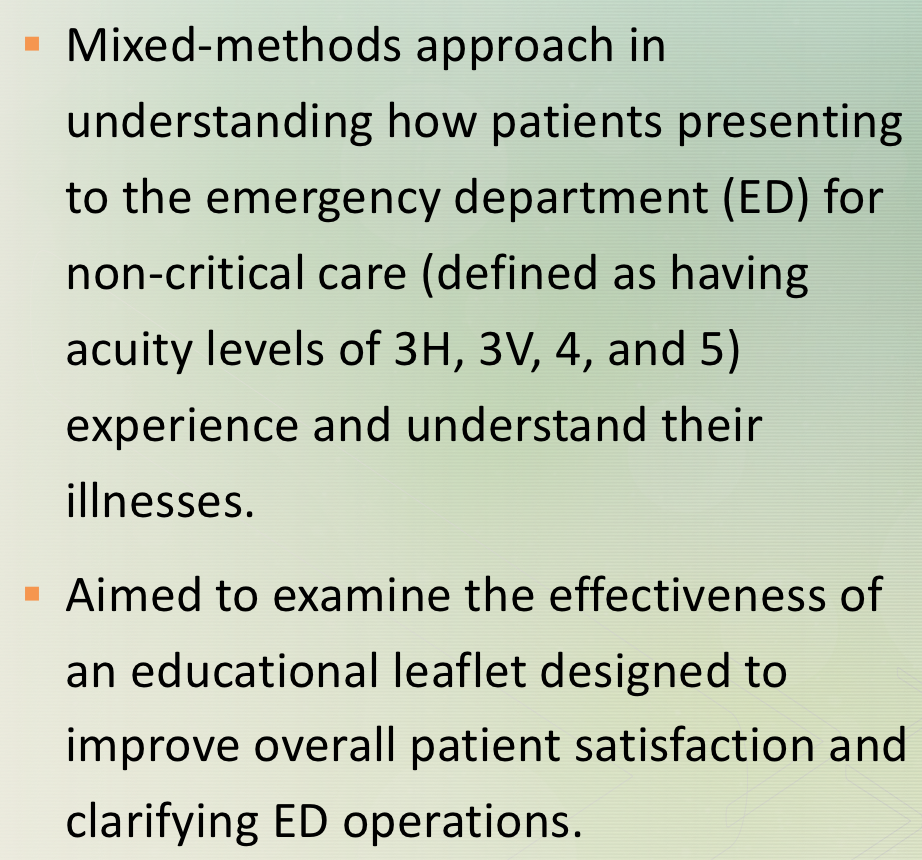
The papers you will hear this afternoon arose from this ongoing work. In the spring of 2015, we designed and co-taught our first iteration of an undergraduate course for pre-medical students, ANT4970 Patient-Physician Interaction. Now on our third rendition, each semester students first spend time shadowing patients and developing a patientcentric lens early in medical training. Student also learn the importance of utilizing mixed-method approaches such as participant observation, semi-structured interviews and quantitative analysis of data, to address questions focused on improving the overall patient experience. This course has had a tremendous impact on undergraduate students who often cite the class as a life changing experience.
Many of those students are now in medical school and Roberta Baer, Seiichi Villalona and I are following them and examining the sustainability of their early patientcentric training as they move through their training. Many students stay with us to complete undergraduate honors theses and we have now expanded our work in the ED to also include anthropology graduate students conducting dissertation research. This approach allows us to position graduate students as experts in patient experience within our institution and also to provide early, sustainable, training in patientcentric care that will, hopefully, be sustained as these trainees become physicians. Ideally, the course can be scaled up to other institutions, positioning med anthro training as a crtical aspect of improving patient experience.
The ability to move a patient satisfaction score from the 50th percentile to the 90th percentile is expensive and difficult. Mainstream medical approaches focus on reinforcing techniques that improve the perception of time spent with the provider during an acute clinical encounter as well as enhanced customer service approaches adopted from customer service friendly business, such as luxury hotel chains and well known amusement parks.
However, the premise of the work you will hear today suggests that those experience improvements may only be possible if specific special populations are better understood and addressed in the ED. The variation in patient visits and patient satisfaction scores is not described in the current Press-Ganey database and might not be well captured in quantitative analysis of large datasets. That is why these papers are critical to advancing our understanding of the patient experience in the ED.
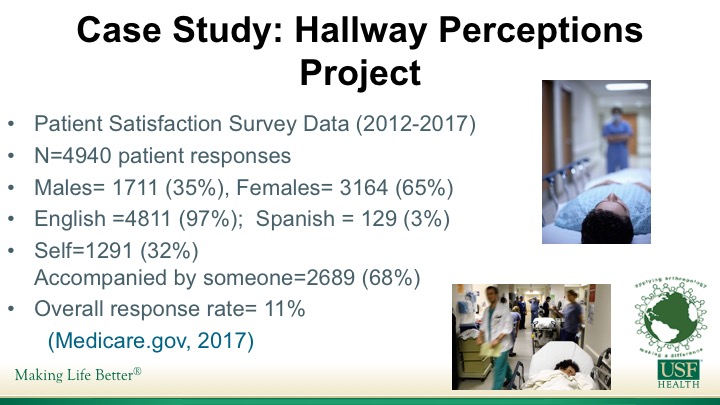
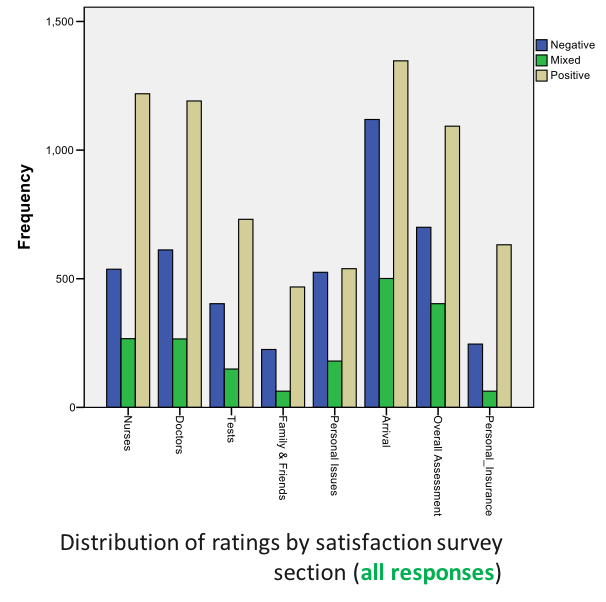
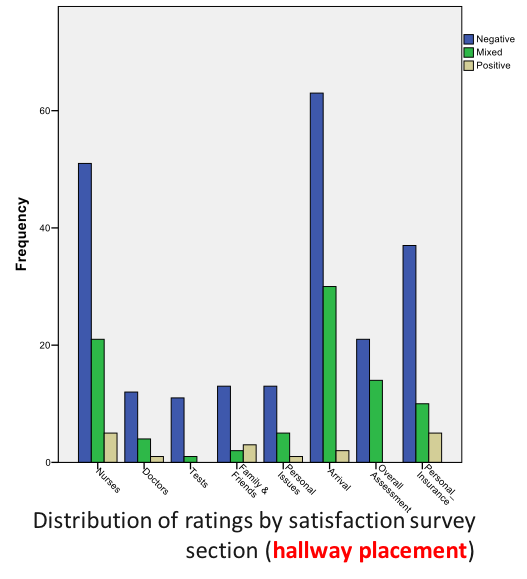
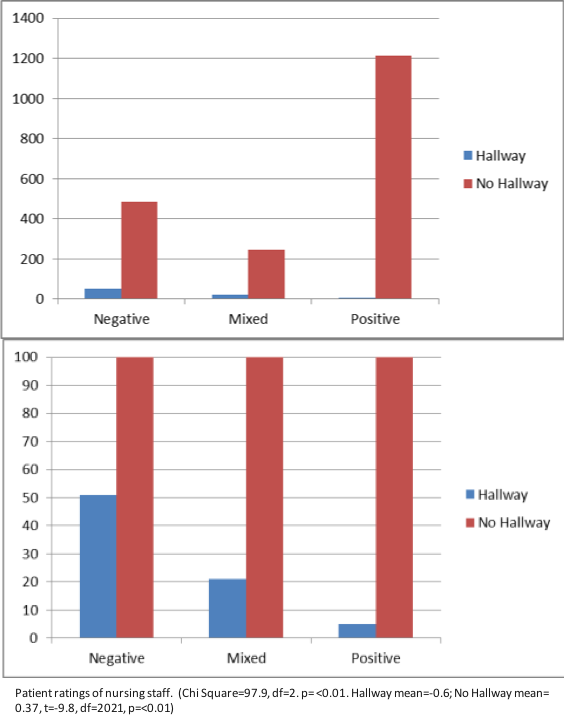
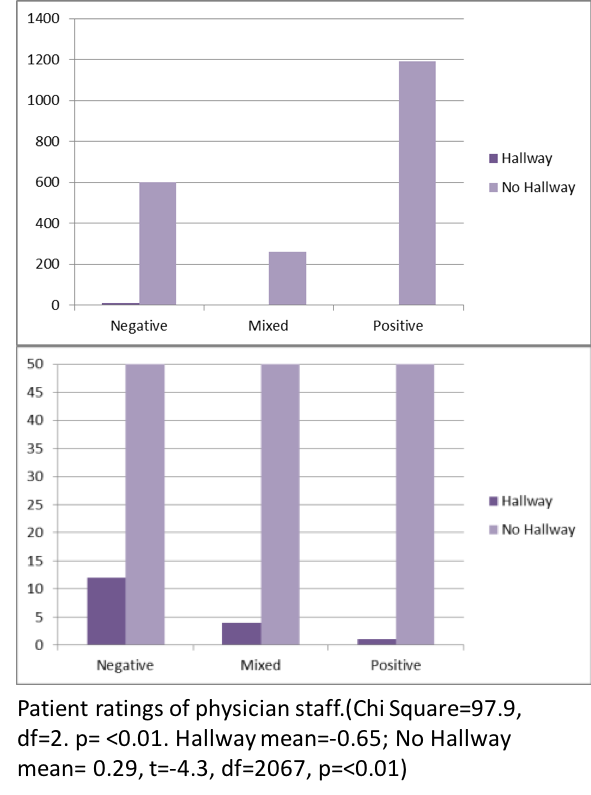
First, you will hear from Seiichi Villalona. Seiichi is a graduate student receiving an MA this semester and moving on to the Robert Wood Johnson Medical School in New Jersey this fall. Seiichi’s work focused on the relationship between placement of patients in less-optimal areas of the ED, such as hallways, and how those circumstances effect the overall experience. Seiichi’s thesis work is on the use of medical interpreters which he conducted with both one of our ED residents as well as another presented today, Mery Yanez Yuncosa who completed her undergraduate honors thesis examining Spanish patients who receive variable translation services in the ED.
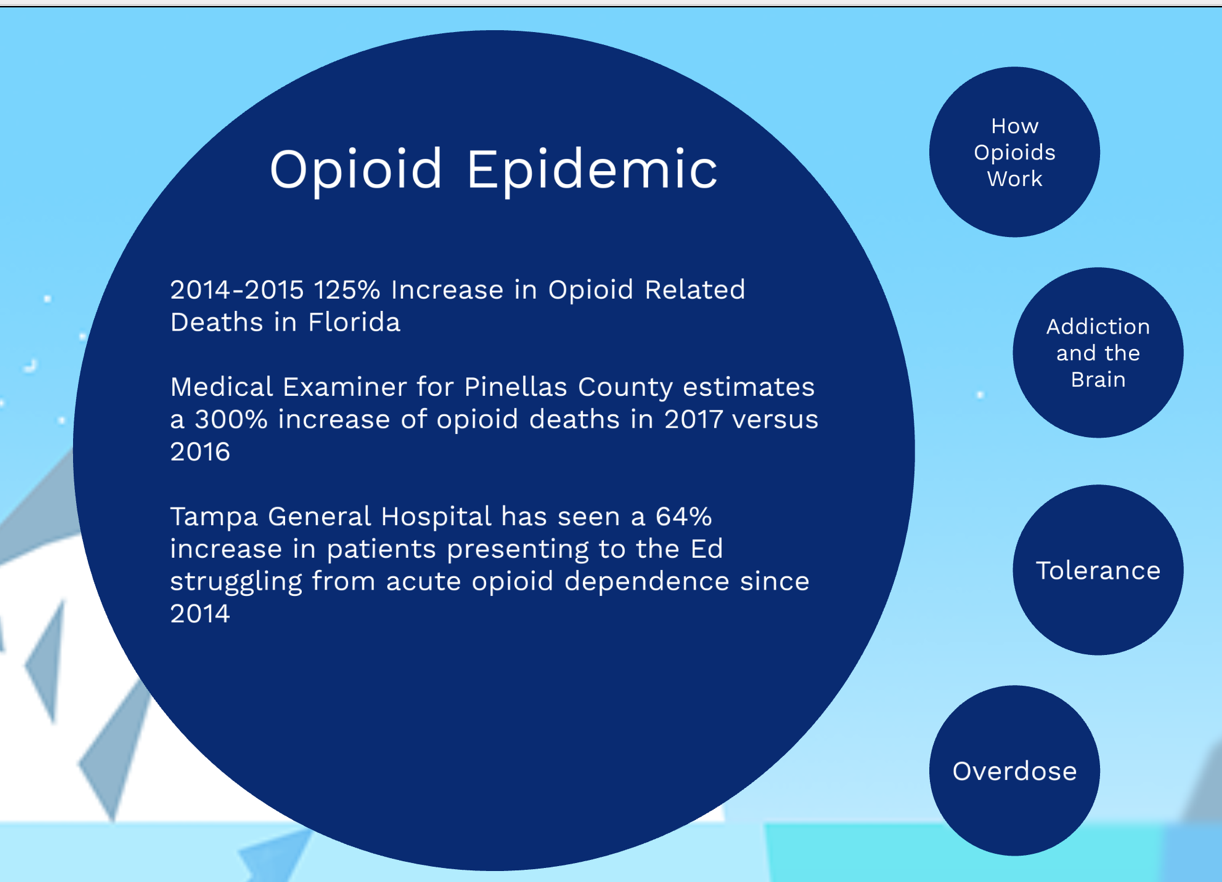
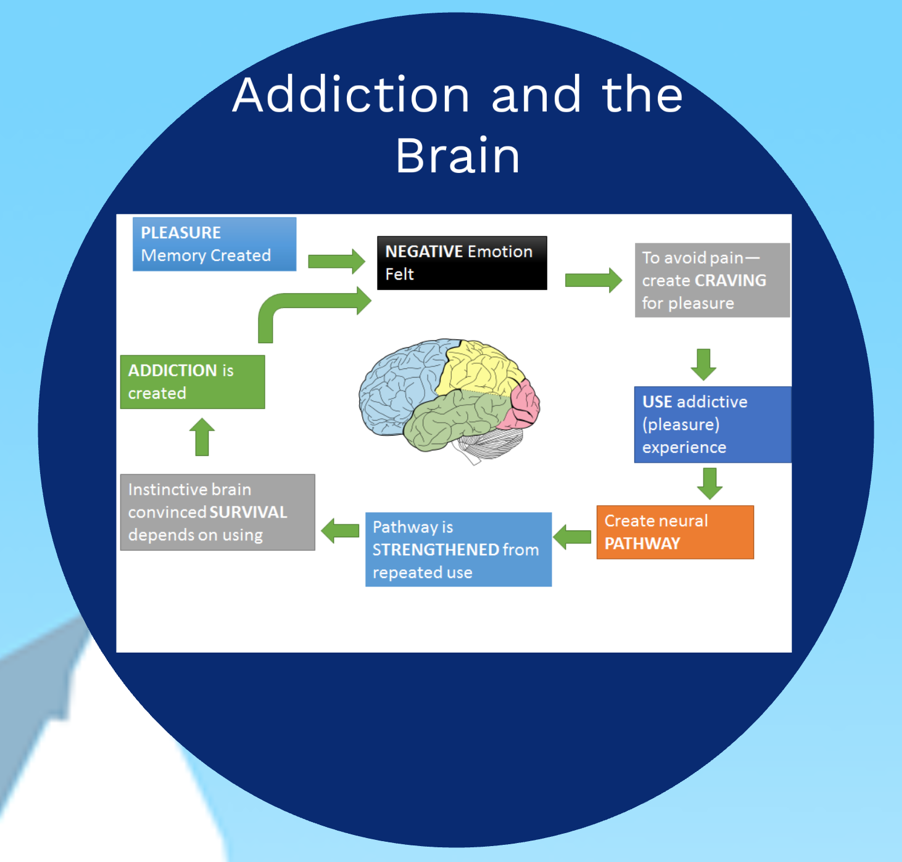
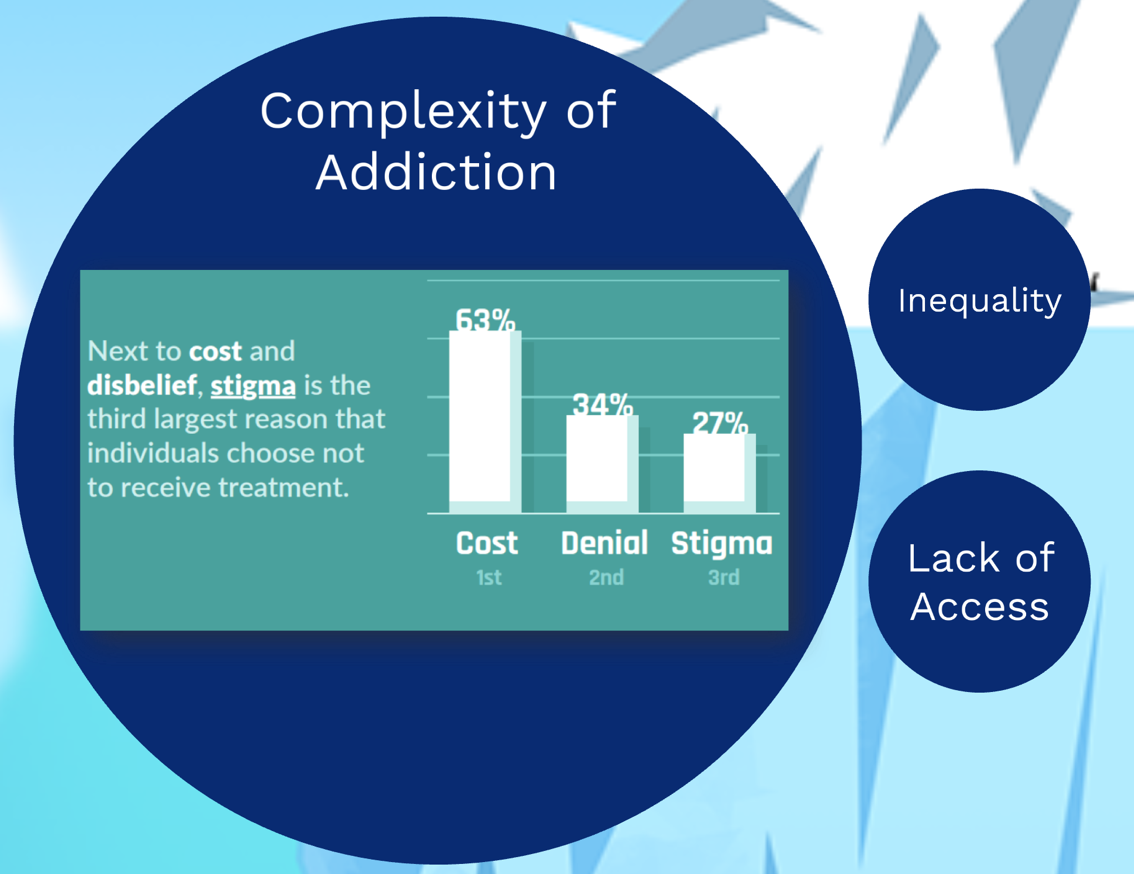
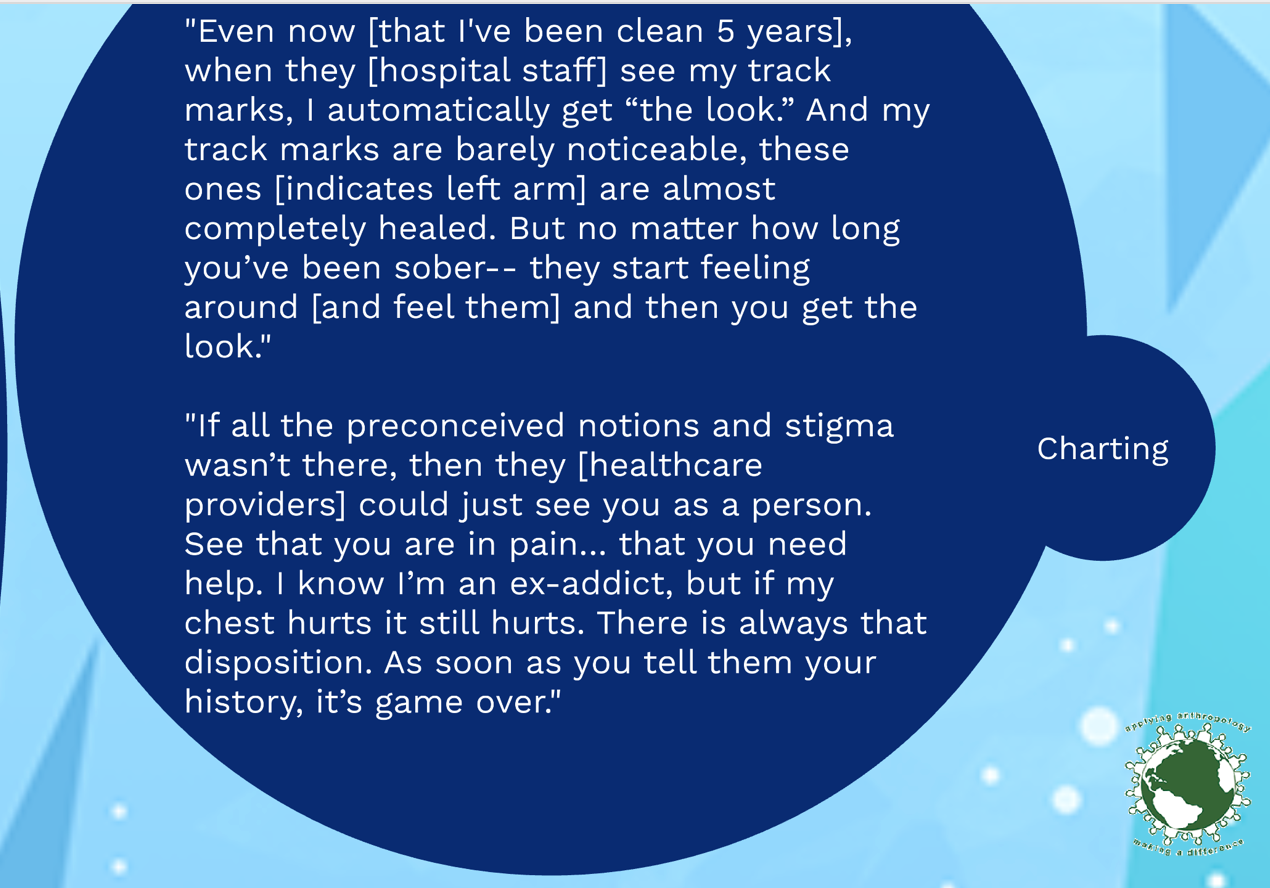
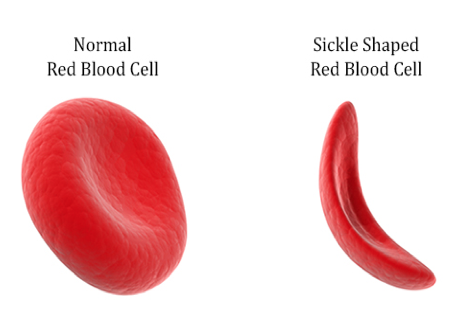
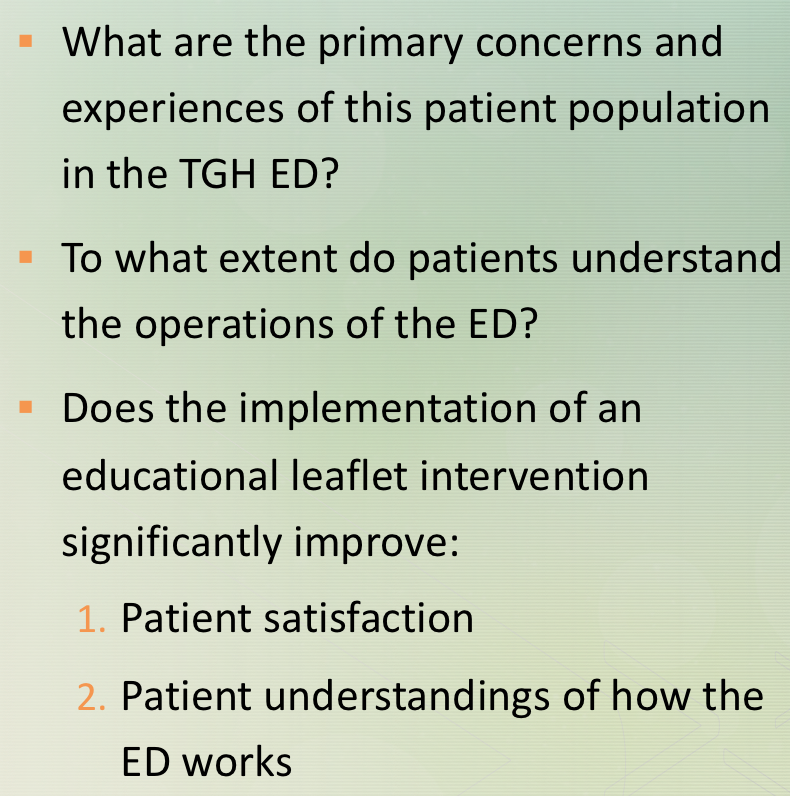
We will also here from another undergraduate student, Killian Kelly, who is planning to eventually move on to graduate school in anthropology and worked with us to develop a patientcentric generated expectations leaflet. In addition, we will hear from Carlos Osorno Cruz who completed his undergraduate degree in anthropology and stayed on in the Emergency Department to continue his work as a research assistant, focusing on ways to improve the care of patients with sickle cell disease patients in the ED. We will also hear from a PhD Student, Heather Henderson, who has recently completed her master degree work on the stigma of opioid addiction. Heather’s work focuses on the medicalization of opioid abuse and how we can work to decrease the marginalization of this population in the ED.
Each presenter will take up to 15 minutes and we will hold questions to the end. After the last presentation, Roberta Baer, the co-designer of this course and these efforts will join us and we will conduct a 15-20 minute discussion and Q&A.
“I was in the hallway the entire time that I was being treated. I do understand that the ER was very busy and I am appreciative that I was seen and treated but I felt invisible most of the time that I was being treated even though I was visible to everyone that walked past. I did not even have a screen up around me and at one point the screen beside my gurney was taken to use for someone else. I do not think I would have minded so much if I would have been asked if I wanted it to be used for me first.” -58 year old female
“Nurses were sitting in station talking about personal matters. I was left in the hallway feeling uncomfortable with other visitors passing by and not being informed of anything.” -57 year old female
YANEZ, Mery and VILLALONA, Seiichi (USF), WILSON, Jason (TGH, USF)
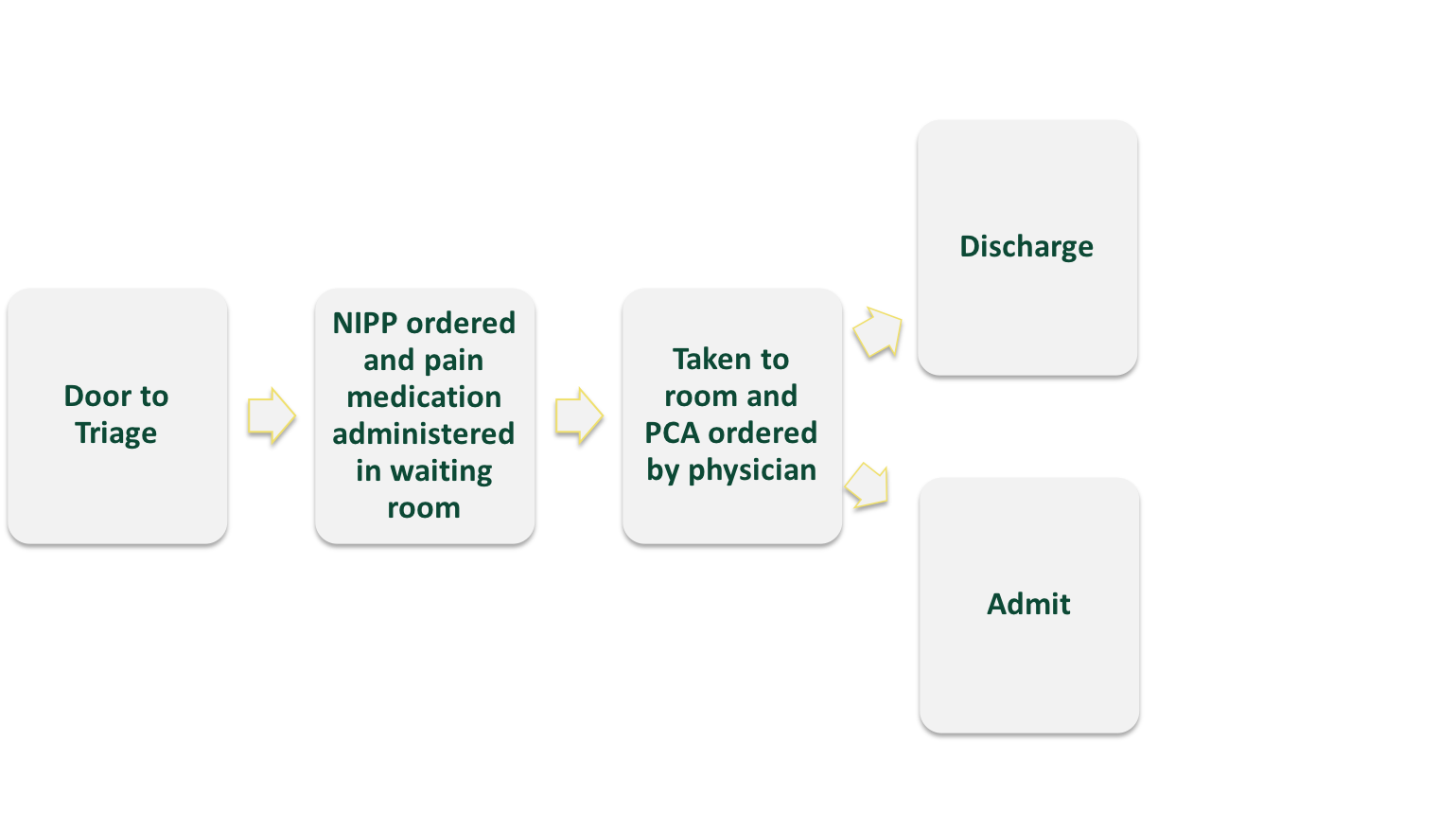
1.Use NIPP approved for SCD Pain Crisis Including Pain Medication (essentially 0% use previous to 2018)
2.Decrease Door to Drug Time. Goal of 30 minutes to pain med (NIPP Utilization while awaiting PCA)
3.Increase PCA use (don’t expect 100% given NIPP use may decrease need for further IV meds)
4.Decrease SCD Pt Admission rate to overall ED admission rate (40%)
5.Decrease ED LOS D/C SCD Pts to 80% of pts D/C in 240 minutes
6.Decrease ED LOS Admit SCD Pts to 80% of pts in 420 minutes
Upcoming Interventions
1.Continue work with hospital VP on educational Video – multi-specialty collaboration for RNs to increase NIPP medication order utilization and acknowledgment of SCD patients
2.TGH Infusion Center and TGH Output Med working with ED to facilitate pathways


















 The papers you will hear this afternoon arose from this ongoing work. In the spring of 2015, we designed and co-taught our first iteration of an undergraduate course for pre-medical students, ANT4970 Patient-Physician Interaction. Now on our third rendition, each semester students first spend time shadowing patients and developing a patientcentric lens early in medical training. Student also learn the importance of utilizing mixed-method approaches such as participant observation, semi-structured interviews and quantitative analysis of data, to address questions focused on improving the overall patient experience. This course has had a tremendous impact on undergraduate students who often cite the class as a life changing experience.
The papers you will hear this afternoon arose from this ongoing work. In the spring of 2015, we designed and co-taught our first iteration of an undergraduate course for pre-medical students, ANT4970 Patient-Physician Interaction. Now on our third rendition, each semester students first spend time shadowing patients and developing a patientcentric lens early in medical training. Student also learn the importance of utilizing mixed-method approaches such as participant observation, semi-structured interviews and quantitative analysis of data, to address questions focused on improving the overall patient experience. This course has had a tremendous impact on undergraduate students who often cite the class as a life changing experience.
 Many of those students are now in medical school and Roberta Baer, Seiichi Villalona and I are following them and examining the sustainability of their early patientcentric training as they move through their training. Many students stay with us to complete undergraduate honors theses and we have now expanded our work in the ED to also include anthropology graduate students conducting dissertation research. This approach allows us to position graduate students as experts in patient experience within our institution and also to provide early, sustainable, training in patientcentric care that will, hopefully, be sustained as these trainees become physicians. Ideally, the course can be scaled up to other institutions, positioning med anthro training as a crtical aspect of improving patient experience.
Many of those students are now in medical school and Roberta Baer, Seiichi Villalona and I are following them and examining the sustainability of their early patientcentric training as they move through their training. Many students stay with us to complete undergraduate honors theses and we have now expanded our work in the ED to also include anthropology graduate students conducting dissertation research. This approach allows us to position graduate students as experts in patient experience within our institution and also to provide early, sustainable, training in patientcentric care that will, hopefully, be sustained as these trainees become physicians. Ideally, the course can be scaled up to other institutions, positioning med anthro training as a crtical aspect of improving patient experience.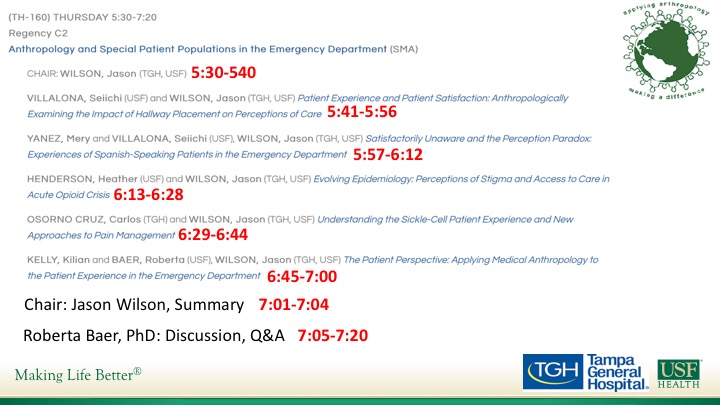
 VILLALONA, Seiichi (USF) and WILSON, Jason (TGH, USF)
VILLALONA, Seiichi (USF) and WILSON, Jason (TGH, USF) 
 YANEZ, Mery and VILLALONA, Seiichi (USF), WILSON, Jason (TGH, USF)
YANEZ, Mery and VILLALONA, Seiichi (USF), WILSON, Jason (TGH, USF)